
Healthcare Disparities
Poverty, a major Social Determinant of Health (SDOH), drives healthcare disparities in the US. Most disparities reports are extensive, complicated, unwieldy, and rely on difficult-to-collect demographic information on each person. We have developed an alternative method that does not require detailed information on each enrollee/person and focuses on income differences rather than differences across racial/ethnic groups.
Assessing with a Quality Index
Health Insurance Disparities Index (HeIDI) was developed by a team from Cornell University’s Brooks School of Public Policy Sloan Program in Health Administration using publicly available data to measure progress in addressing healthcare disparities between high- and low-income people. Since type of health insurance is driven by socioeconomic status, comparing quality of care performance and identifying disparities between Commercial/Private HMOs and Medicaid HMOs is an appropriate complement to DEI-based approaches.
Criteria Used for HeIDI Measurement Selection
The original portfolio of HeIDI HEDIS® metrics used for Measurement Years 2017 through 2024 consisted of HEDIS® measures which were selected upon meeting the following criteria (https://doi.org/10.37765/ajmc.2025.89701):
Any measures used for public performance reporting and/or in VBP quality programs impacting ≥ 50% of State Medicaid MCO program enrollees nationally is automatically included as a HeIDI measure.
Any measure endorsed by more than two nationally recognized authoritative entities (NCQA, CMS, NQF, or CQMC) as a disparities measure and/or for public reporting is designated as a HeIDI measure.
If a measure is used for public performance reporting and/or in VBP quality programs impacting ≥ 30% but < 50% of State Medicaid MCO program enrollees nationally, it is considered equivalent to one nationally recognized authoritative entity endorsement and qualifies as a HeIDI measure under the above rule.
Starting with Measurement Year 2025 (Reporting Year 2026) and beyond, the portfolio of HeIDI HEDIS® measures will be consistent with and henceforth will be adjusted solely to reflect those measures that are in common for both Commercial and Medicaid HMOs used for achieving NCQA Health Plan Accreditation (HPA) and/or Health Plan Ratings (https://www.ncqa.org/hedis/health-plan-ratings/). This approach has been adopted for several reasons. Nearly all Commercial HMOs pursue NCQA HPA and thus must provide NCQA with their performance of these measures which are then publicly reported. Similarly, the vast majority of States (reflecting most of the national Medicaid managed care enrollment) now require their respective Medicaid HMOs to achieve NCQA HPA which results in these health plans likewise reporting their performance for these same measures. Using this measure selection approach ensures maximal public reporting of the HeIDI HEDIS measures and allows for consistency of reporting whenever NCQA adds or removes any measures. Consequently, any such changes are now reflected in the HeIDI HEDIS® portfolios for Measurement Years 2025 and 2026.
HeIDI Measurements and Weights Used for Each Measurement Year
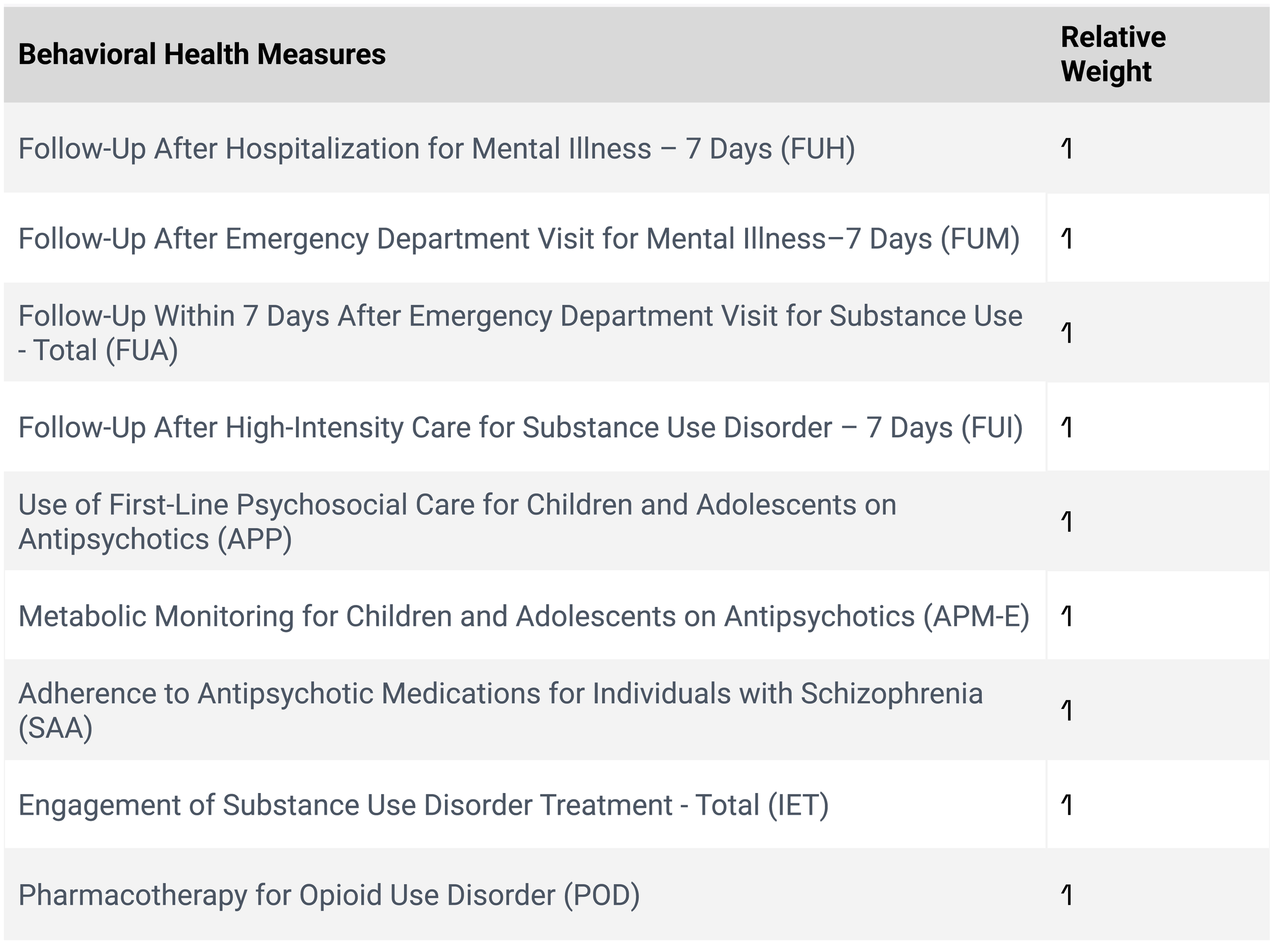
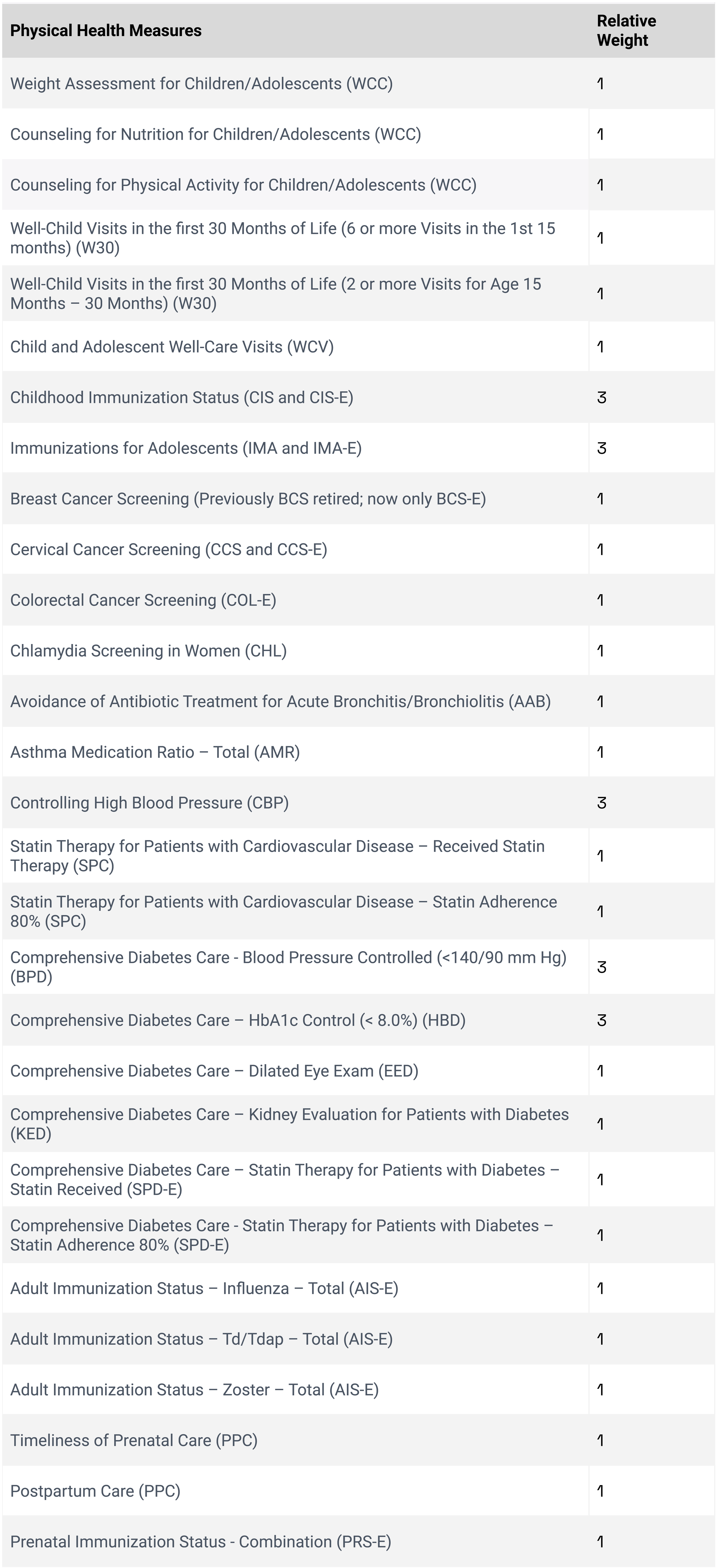
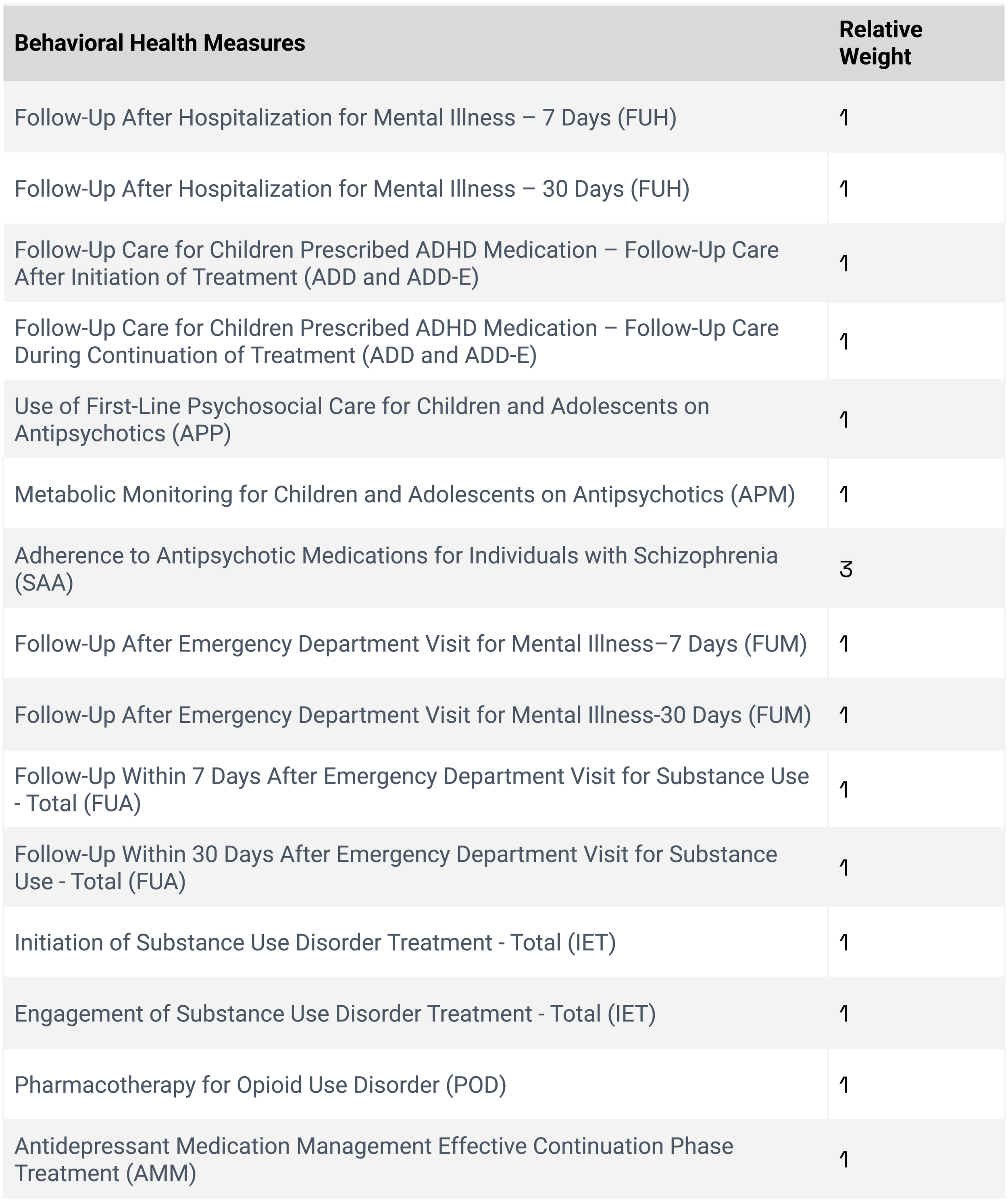
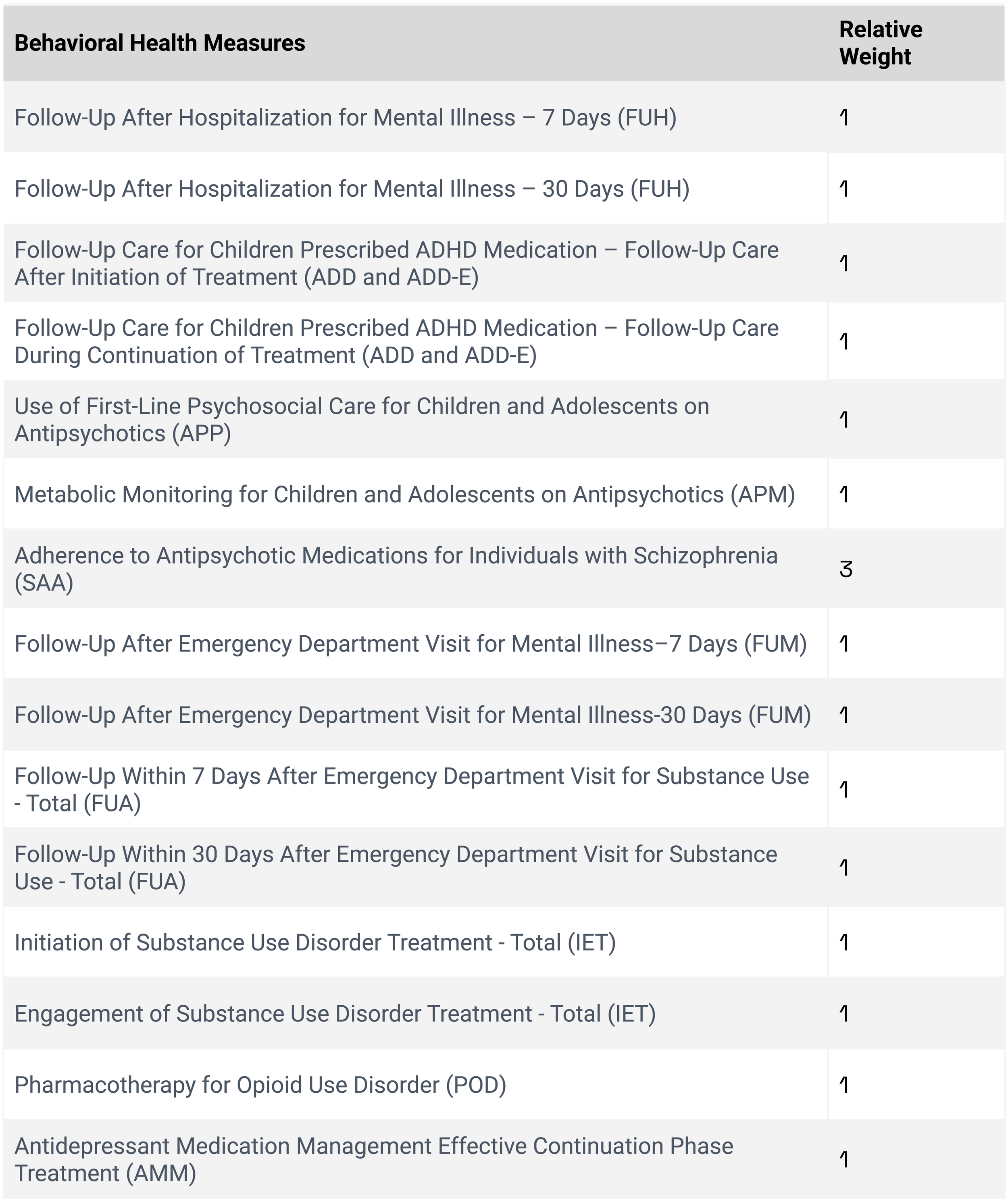
HeIDI Measures and Weights for HEDIS Reporting Year 2027 (Measurement Year 2026)

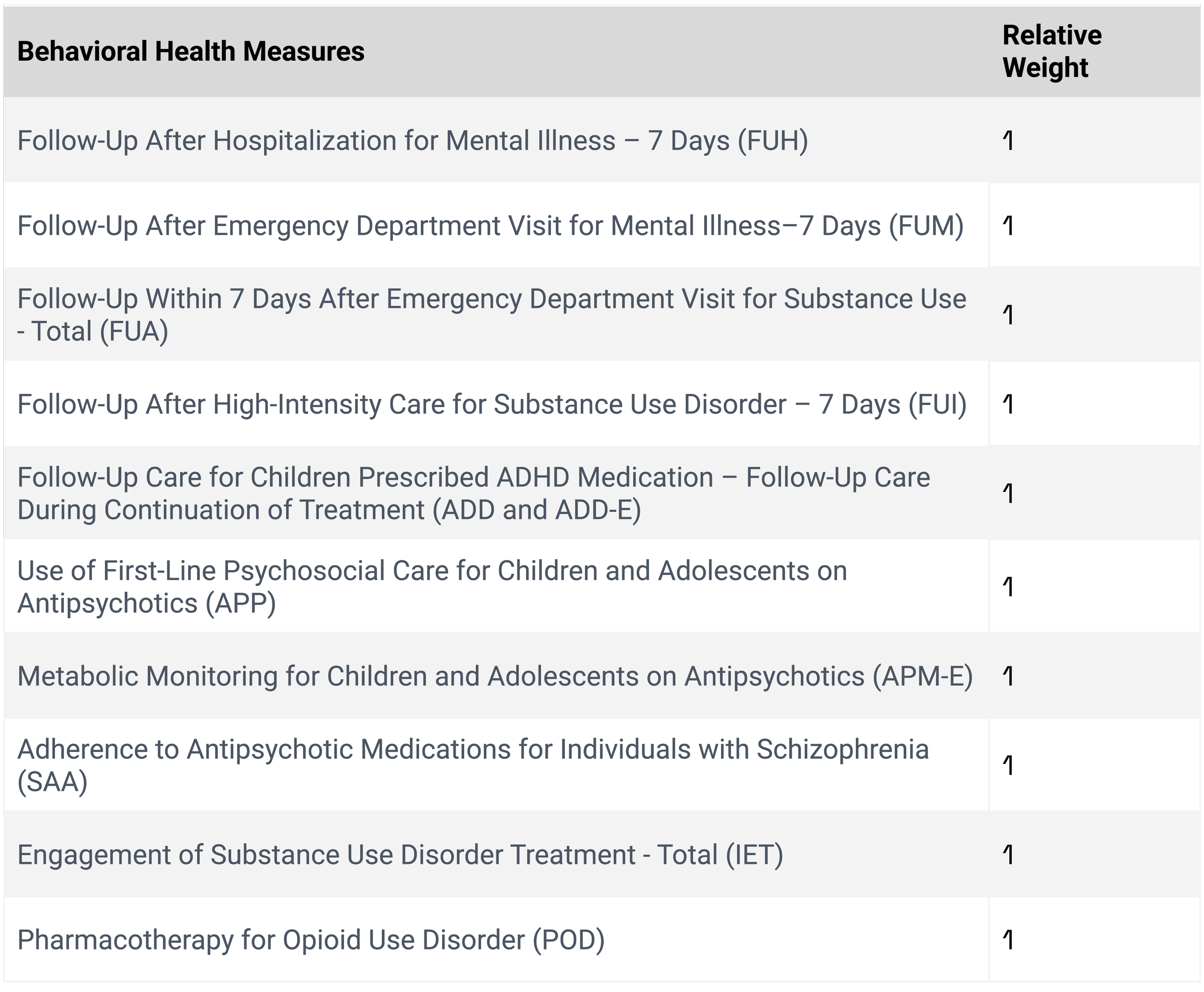
HeIDI Measures and Weights for HEDIS Reporting Year 2026 (Measurement Year 2025)
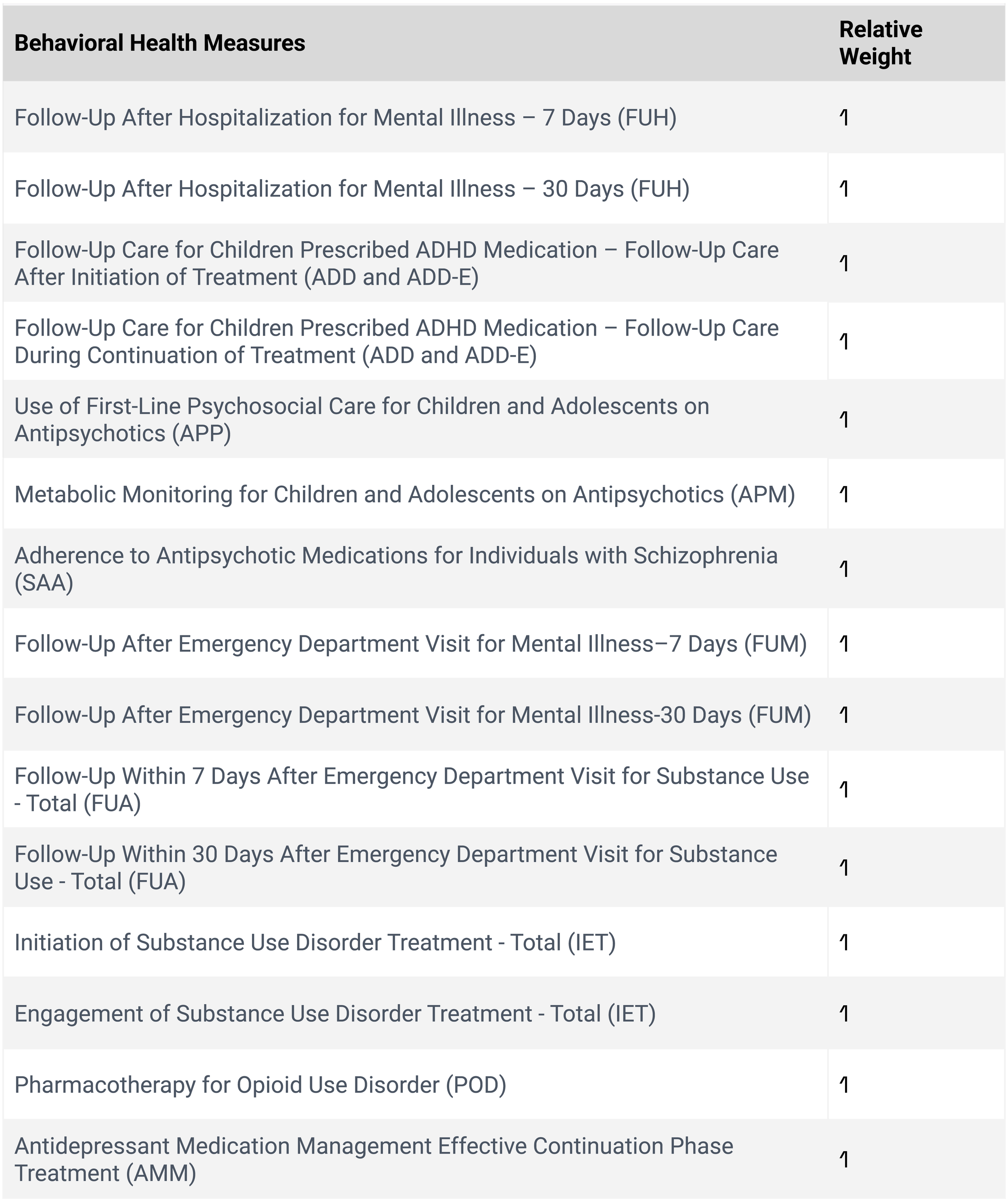
HeIDI Measures and Weights for HEDIS Reporting Year 2025 (Measurement Year 2024)

HeIDI Measures and Weights for HEDIS Reporting Year 2024 (Measurement Year 2023)

HeIDI Measures and Weights for HEDIS Reporting Year 2023 (Measurement Year 2022)

Formula
HeIDI index in year t = ∑ ([(Cᵢ–Mᵢ) × wᵢ] × I[Cᵢ > Mᵢ]) / (∑ wᵢ × Cᵢ)
where Cᵢ and Mᵢ represent the average performance of commercial and Medicaid plans nationally, respectively, for measure i in year t; wᵢ is a weight equal to 1 when i is a process measure and 3 when i is an outcome measure; and I(Cᵢ > Mᵢ) is an indicator function that equals 1 when Cᵢ is greater than Mᵢ and 0 otherwise. Each performance measure is measured as the percentage of patients in a type of plan who receive the recommended medical care or achieve the recommended outcome, where a higher value indicates superior medical care, on average, for the enrollees.
For comparisons between commercial and Medicaid plans that have behavioral health services included in the benefit package for enrollees, portfolio of measures include both physical and behavioral health measures in the HeIDI calculations. When comparisons are being made where behavioral health services are carved-out of the benefit package, consider utilizing the Non-Behavioral Health (NBH) HeIDI methodology which excludes the behavioral health measures in the portfolio.
Reported and Most Current HeIDI Results
A positive score: commercial enrollees are receiving higher quality care.
HeIDI demonstrated (using the Standard and the Non-Behavioral Health Tools) a gradual worsening of disparities (the higher the value, the poorer the performance) nationally with a substantial deterioration during the COVID-19 pandemic years between individuals with Commercial/Private and Medicaid managed care from 2017 to 2022. The HeIDI improved slightly in 2023 with improvement for 2024 which brought its performance to that witnessed during 2020 (at the start of the COVID-19 pandemic).
Summary of Potential Benefits in Using HeIDI
HeIDI is a practical tool for assessing progress in addressing and eliminating healthcare disparities between different insurance product lines.
Since HeIDI is based on socioeconomic differences between population groups, it is an appropriate alternative method to DEI-based approaches.
Since health insurance is driven by socioeconomic status, comparing quality of care performance and identifying disparities between Commercial/Private HMOs and Medicaid HMOs is an appropriate alternative to DEI-based approaches.
HeIDI can allow health systems researchers to explore various underlying variables contributing to the performance of an entity (such as states, health plans, delivery systems), including the impact of carved-out services, health plan size, tax status of organizations, state eligibility rules, benefits provided, waiver programs, financial incentives, implementation of alternative payment mechanisms, existence of “sister” Commercial/Private plans alongside Medicaid, and regional characteristics.
LATEST NEWS
On November 11, 2025, the American Journal of Managed Care posted our study, “Assessing New York’s Health Care Disparities Using Health Plan Quality Data”.
Using the newly developed Health Insurance Disparities Index, we found that New York’s Medicaid health maintenance organizations (HMOs) outperformed Medicaid HMOs nationally in closing the gap for health care disparities by enrollee income. Additionally, New York’s Medicaid Health and Recovery Plans for severely mentally ill Medicaid beneficiaries also outperformed mainstream Medicaid HMOs in other states. The following characteristics of New York’s approach for managing Medicaid managed care could explain its strong performance:
Value-based payment and quality incentive programs
Waiver programs
Eligibility and benefit design
Integration of physical health services with behavioral health
Health plan characteristics
Peer-Reviewed HeIDI Publications
Stankaitis JA, Pham H, Singh S, and Nicholson S. Assessing New York’s health care disparities using health plan quality data. American Journal of Managed Care. 2026;32(5): e167-e174: https://www.ajmc.com/view/addressing-health-care-disparities-using-a-health-plan-quality-measures-index
Stankaitis JA, Singh S, and Nicholson S. Assessing healthcare disparities using a health plan quality measures index. American Journal of Managed Care. 2025;31(9): 468-475. https://doi.org/10.37765/ajmc.2025.89701. Originally online publication on February 26, 2025: https://www.ajmc.com/view/addressing-health-care-disparities-using-a-health-plan-quality-measures-index